
Table of Contents
The Lockdown Madness
On March 16, 2020, four days after the World Health Organization (WHO) declared COVID‑19 to be global pandemic, Neil M. Ferguson and colleagues at Imperial College London, in collaboration with the WHO, published a modeling paper advocating strict “mitigation policies” ostensibly to limit the spread of SARS‑CoV‑2, the novel coronavirus that causes the disease.
That paper was highly influential and was cited by governments around the world, including the United Kingdom and the United States, as justification for implementation of authoritarian “lockdown” measures including business closures, school closures, stay-at-home orders, and mask mandates.
These lockdown measures were sold to the public based on the lie that they would be strictly temporary, just “two weeks to flatten the curve”—or, in White House parlance, “fifteen days to slow the spread”.
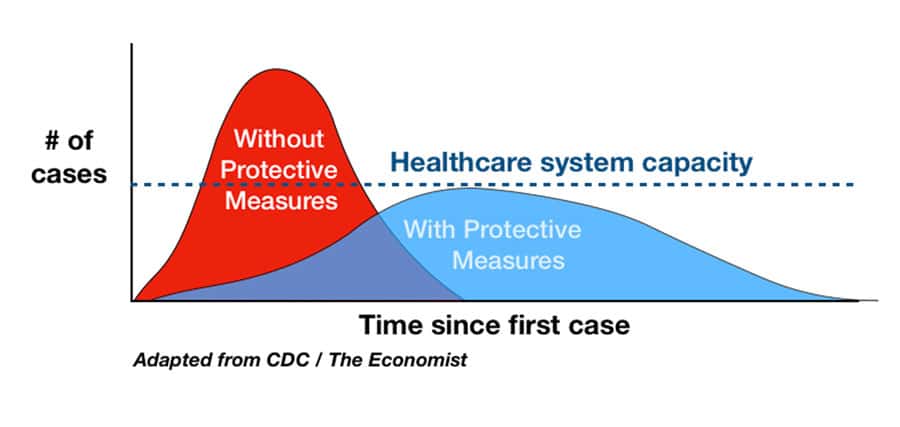
“Flattening the curve” meant to slow the spread enough to give hospitals time to ramp up capacity and obtain supplies so that they wouldn’t become overwhelmed with COVID‑19 patients. This concept was graphically explained to the public by the lockdown-loving New York Times with the following graph:
But it was all a lie. The lockdown measures were never intended to remain in place for only two weeks. This is obvious from the fact that the Imperial College modelers advocated maintaining lockdowns until a vaccine could be developed and essentially forced upon the population.
Indeed, coerced mass vaccination is precisely what occurred once the US Food and Drug Administration (FDA) granted emergency use authorization (EUA) for the mRNA COVID‑19 vaccines.
The government systematically violated individuals’ right to informed consent by (a) deceiving people into willingly accept injection with these experimental pharmaceutical products and, failing success in that endeavor, (b) coercing people into getting vaccinated against their will.
The government lied to the public about practically everything, but, in particular, the vaccines were sold to the public on the basis of the lie that two doses would confer durable sterilizing immunity, thereby enabling “herd immunity” to be reached by stopping infection and transmission.
For those who weren’t deceived by false claims about the safety and effectiveness of these products, the government delivered the clear message that their freedom would remain curtailed and their ability to make a living threatened unless and until they got vaccinated—even if they had already acquired the superior immunity conferred by infection.
Policymakers implementing lockdown measures pretended to care about human lives, but we know they were really more concerned with exercising power and control over others because, just as their political calculations ignored natural immunity, they never factored the costs and predictable harms of the measures they were advocating into their thinking.
Indeed, the Imperial College modelers admitted that they “do not consider the ethical or economic implications” of the lockdown measures they advocated.
Dr. Anthony Fauci, the Director of the National Institute of Allergy and Infectious Diseases (NIAID) under the National Institutes of Health (NIH) and a top advisor to the president on the White House’s coronavirus task force, similarly admitted that he wasn’t considering the costs of the lockdowns. “I don’t give advice about economic things,” he said. “I don’t give advice about anything other than public health.”
Tellingly, the rationale for the lockdowns quickly shifted from being short-term measures to “flatten the curve” by spreading out the number of newinfections over time, with the areaunder bothhypothetical curves being the same, to being long-term measures supposedly capable of not merely delaying but stopping community transmission.
In other words, under the original rationale for the measures being temporary, the only deaths hypothetically prevented were those that would otherwise occur due to people being unable to get hospital care, whereas the new rationale for the measures persisting indefinitely was that this would reduce the total number of “cases”—the official counting of which was characterized by institutionalized scientific fraud.
There was no scientific basis for this shift in rationale whereby the lockdowns were maintained on the grounds that they would reduce total case numbers. Instead, it was a faith-based policy. Policymakers deliberately shut down the economy based on the hope that this would stop community transmission and the hope that the population could ultimately be saved by mass vaccination.
That the policies were based on “hope that the vaccines would work” the way that government officials falsely claimed they would has been acknowledged in Congressional testimony by Dr. Deborah Birx, the former White House Coronavirus Response Coordinator. (Birx later claimed that she had always known that the vaccines would not prevent transmission, which is enlightening given the fact that she was among the government officials claiming that they would stop infection and transmission.)
The fact that the policy was faith-based has also been admitted by then CDC Director Rochelle Walensky. Commenting on the vast disparity between what government officials told the public and how the vaccines actually performed, she attributed it to officials like her having “wanted to be hopeful”. (Far from accepting responsibility for having deceived the public, however, she went on to essentially blame the public for taking the government’s claims at face value.)
The promised benefits of the lockdowns, of course, never manifested in the data. This includes, as recently acknowledged by Anthony Fauci, the evidence-less claim that mandatory use of masks in public places would prevent community spread.
The harms caused by these authoritarian policies, on the other hand, have incontrovertibly been devastating, with the burden of harms being disproportionately borne by children, who happen to be at very low risk from COVID‑19.

Great well presented and timely article for all to read. Thank you!
JB,
Glad you found it useful! Thanks for the feedback.
Asymptomatic transmission happens all the time and cannot be stopped any more than we can stop the ocean tides. The PCR test proved that. Millions of people tested positive for the presence of viral genetic material and never displayed a single symptom. The particles transmit, the symptoms don’t. Whether a person displays symptoms or not depends more on the condition of their immune system than the presence of the virus. Trying to eliminate the virus is a battle between God’s natural design and man than man cannot win. Man must learn about how the immune system works, where the protection of infection is, and how to bolster that cellular protection that does not rely on the creation of serum antibodies from injections.
Kevin,
With respect, it is evident to me from your comment that you didn’t read the article before commenting. The article explains why your belief that the PCR test proved that asymptomatic transmission occurs all the time is incorrect, so I do encourage you to read it.
The PCR test is indeed a bad example due to high false positive rates and nonstandard cycling. Trying to use any test to determine the levels of contagiousness based on viral loads is complicated. The simple point I was trying to make is that you can find viral genetic material in the mucosa of people who are ill, and people who are not ill. We are exposed to pathogens all the time, the source of which can be the environment, shedding from people who are ill, transmission in the atmosphere from people who are infected but not displaying symptoms, and exchange from people who are not infected at all. The pathogens always move between us, the symptoms don’t.
I appreciate that clarification, Kevin, and you are certainly right to emphasize the distinction between infection and disease (as I also do in the above article), but it still appears to me that you have not read the article since the human challenge study I discuss showed that individuals’ viral loads were indicative of viral shedding mostly after symptom onset. Only 7% of shedding occurred during the presymptomatic phase of infection.
I did read it, several times. Viral loads fluctuate for sure depending upon whether the person doing the shedding is infected and presymptomatic, asymptomatic, or symptomatic. So, where’d ya get that virus? Hard to say.
Kevin, I have shown you the best study to date for understanding viral loads and viral shedding, and it supports my conclusion. If you are going to insist that my conclusion is incorrect, please show me where I got any facts wrong or employed any logical fallacies, and also support your opposing conclusion with scientific evidence.
We are in agreement that “silent spreading” is not the major driver in community transmission.
Oh! Thanks for that clarification. I thought when you said that “asymptomatic transmission happens all the time” that you were disagreeing with my article’s conclusion.
Thanks for this great text (and I love its length and richness of details). While I am not claiming to have seen every nuance of the c19 “dissident” discussion, my personal view is that the issues of how important (or un-important) asymptomatic and presymptomatic transmission are have not been discussed sufficiently before. I am only a chemist, not a biologist (and hence “not an expert”), but to me a low importance of asymptomatic/presymptomatic spread makes much more sense than the official claim that these were the true c19 pandemic drivers. After all, in contrast to bacteria, viruses cannot multiply by themselves, they need the biochemical machinery of living cells (cells of my body) for that, leading to these cells being killed (by total viral capture, or by the immune system) or at least being severely impaired in their functions. And although in some abstract sense one single virus particle may be sufficient to infect someone else, I do hear and understand the message that the viral load has to be quite high to really become infected (for various reasons, among them cross-immunity, and the probability of a virus particle successfully entering a cell and overtaking its machinery being much less than 100% upon contact, etc.). In other words, to be infectious to others I have to produce LOTS of fully functional viral particles, which means that lots of my cells have to die or become seriously incapacitated. I will notice that as “symptoms”. — This is a believable “mechanism story”. The asymptomatic/presymptomatic story fails to deliver a plausible mechanism, i.e., it is a bare claim, without sufficient biochemical background, in flat contradiction to the “follow the science” mantra.
Bernd,
Thanks for sharing that insight. It makes perfect sense to me, and it is known that dose and duration of exposure is a risk factor for more severe symptoms.