
Table of Contents
Introduction
In October 2020, two months before the Food and Drug Administration (FDA) first granted emergency use authorization for COVID-19 vaccines, Dr. Rochelle Walensky, who went on to become director of the Centers for Disease Control and Prevention (CDC) under the Biden administration, claimed that vaccines would be needed to achieve herd immunity because “there is no evidence for lasting protective immunity to SARS-CoV-2 following natural infection”.
That was a lie.
At the time Walensky made that bold statement, studies had already shown that, in addition to effective cellular immune responses, neutralizing antibodies induced by infection were persistent in the blood of almost all people who recovered. Additionally, it was known that infection induced memory responses, with indications of the induction of long-lived bone marrow plasma cells—a known immunologic marker of long-term immunity—that could rapidly churn out more antibodies in the event of reexposure to SARS-CoV-2, the coronavirus that causes COVID-19.
The claim that the vaccines would confer herd immunity by stopping infection and transmission and thereby bring the pandemic to an end proved to be a false promise. The induced sterilizing immunity, or ability of circulating antibodies to stop infection, wanes rapidly so that fully vaccinated people can become infected and spread the virus to others.
Walensky herself publicly admitted this in August 2021 after CDC researchers had learned that 74% of COVID-19 cases in a large outbreak in Massachusetts were fully vaccinated people and that the amount of virus shed by vaccinated people was just as high as that of the unvaccinated, suggesting equal contagiousness. (It was this finding that prompted the CDC to reverse its mask guidance, shifting from telling fully vaccinated people that they no longer needed to wear a mask to telling them that they needed to mask up once again.)
After the FDA issued emergency use authorization for COVID-19 vaccines in December 2020, the CDC claimed that the available evidence indicated that natural immunity was short-lived.
That, again, was a demonstrable lie.
That falsehood was eventually removed from the CDC’s website only to be replaced with a recommendation for people who’ve recovered from infection to still get vaccinated on the grounds that the duration of natural immunity remained unknown.
Thus, while no longer outright lying, the CDC continued to deceive the public by deliberately withholding the fact that studies had shown that infection was likely to induce long-term immunity.
Indeed, in May 2021, scientists confirmed that infection induced differentiation of memory B cells into long-lived bone marrow plasma cells, an immunological marker of long-term immunity. Yet the CDC persisted in its deceitful message that even people who already recovered from infection needed to get fully vaccinated on the implicit grounds that natural immunity might be short-lived.
Then, in August 2021, the CDC went even further by explicitly claiming that the evidence suggested that “people get better protection by being fully vaccinated compared with having had COVID-19.”
That was yet another outright lie, even more egregious than the CDC’s earlier disinformation.
In fact, by that time, studies had overwhelmingly shown natural immunity to be both broader and more durable than the immunity induced by vaccines.
The CDC continued lying that natural immunity was inferior until December 3, 2021, when that disinformation, like its original disinformation about natural immunity being short-lived, was removed from its website.
Nevertheless, the CDC to this day persists in telling the public that natural immunity may or may not offer only “some” protection, in comparison to COVID-19 vaccines that “are effective at preventing COVID-19”.
Additionally, on January 15, 2021, the CDC started telling people with natural immunity that they, too, should get fully vaccinated on the grounds that this would provide them with an additional protective benefit beyond the protection afforded by natural immunity alone. To this day, the CDC persists in telling people who already have natural immunity that getting vaccinated “provides added protection to your immune system.”
However, a study by CDC researchers published on January 19, 2022, in the CDC’s Morbidity and Mortality Weekly Report (MMWR) not only shows incontrovertibly that natural immunity offered better protection than vaccine-induced immunity against the Delta variant of SARS-CoV-2, but also challenges the assumption—never studied in clinical trials—that vaccination after recovery from infection offers such a substantial additional benefit that it clearly outweighs the risks from these pharmaceutical products.
In fact, the claim that the data show that the vaccines confer a substantial additional benefit in protection against COVID-19 is conspicuously absent from the new CDC study.
What the CDC’s Own Data Tell Us About Natural vs. Vaccine-Induced Immunity
A picture speaks a thousand words, so let’s start by looking at two key graphs contained in the supplementary materials (not in the main paper) showing clearly how unvaccinated people with natural immunity fared better than people who were fully vaccinated (the first graph showing data from California and the second from New York).
To understand what you’re about to see: the lines on these graphs show the risk of being identified as a “laboratory-confirmed COVID-19 case” (i.e., receiving a positive PCR test) expressed as an estimated hazard rate (the rate of lab-confirmed cases per 100,000 person-days at risk). Don’t worry about not understanding this methodology; all you need to know is that higher up along the y-axis means greater risk, and the x-axis represents time from May 30 into November 2021.
There are four lines: (1) the solid dark blue line shows the risk for unvaccinated people without evidence of prior infection, or people who were immunologically naïve; (2) the dotted blue line represents vaccinated people without evidence of prior infection, or people with vaccine-induced immunity; (3) the dotted light blue line represents unvaccinated people with evidence of prior infection, or people with natural immunity; (4) the dotted black line represents vaccinated people with evidence of prior infection, or people with so-called “hybrid immunity”.
Here's what the respective data from California and New York show:

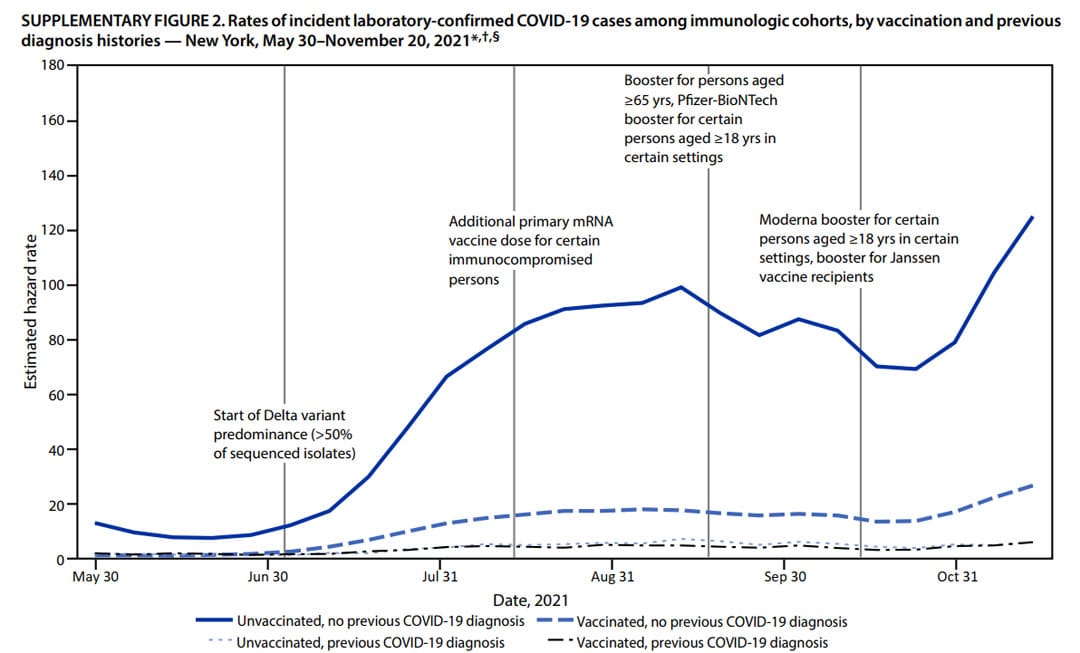
As you can see, unsurprisingly, by far the highest risk of receiving a positive PCR test was associated with being immunologically naïve. By comparison, the risk was far lower for people who were fully vaccinated.
However, even greater protection was offered by the immunity induced by infection, with or without vaccination.
In other words, the CDC’s own data falsify the claim that the CDC started making in August 2021 that the immunity induced by COVID-19 vaccines is superior to natural immunity.
Note that this result holds true even though their methodology biased the study in favor of finding comparably greater protection amongst the vaccinated.

Thank you for using that nasty word (lie) so seldom associated with government activity. Their euphemisms, usually intended to cover up their malfeasance, are so transparent as to be ludicrous.
Sometimes you just gotta tell it like it is!
Kudos Jeremy. …as usual very thorough.
Pandemic Logic Cheat-sheet Syllogism:
We must do something:
X is something.
So we must do X.
Circular:
X is desirable because X works.
We know X works because X is desirable.
Post-Hoc:
X is followed by desired outcome. Continue X.
X not followed by desired outcome. Increase X.
Excellent cheat sheet!
So infection confers immunity across variants? Many ask about that.
Yes. Variants can “escape” sterilizing immunity, meaning protection against infection due to circulating antibodies, to one extent or another. People with natural immunity may become reinfected. The cellular immunity that is induced with natural immunity is protective across variants, so that a reinfection with an escape variant is more likely to be asymptomatic or mild.
Hello, it seems to be a very good article, but even being a unvaccinated and having published on the subject during the two years of the pandemic, I cannot go through these long messages, that say again and again that we were lied to constantly during the pandemic, by the public authorities in charge of protecting us and nothing happens. The public has given up control of their lives and the authorities, I feel, can do what they want, under the guidance of the rich and powerful. Gazoline at over $2 a liter in Canada is one sure sign and the price of food are hitting the weakest the hardest and no one will step up for them. Sad times with no end in sight.
We have to keep fighting. If you can think of anyone who might be reached by this article, please share it with them.